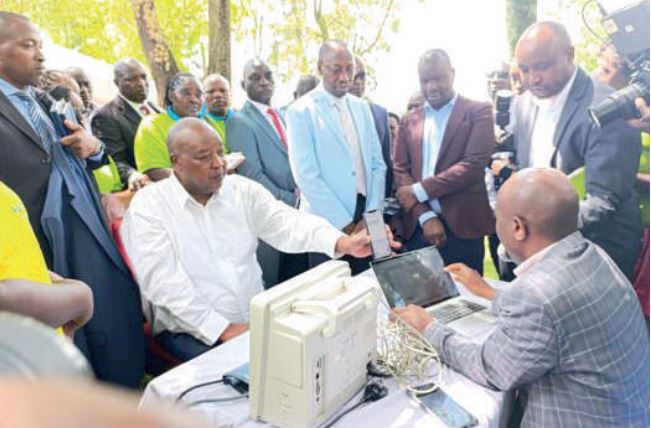
 Governor Amos Nyaribo during a mass registration drive for Nyamira residents into Social Health Authority platform /KNA
Governor Amos Nyaribo during a mass registration drive for Nyamira residents into Social Health Authority platform /KNA
Kenya’s transition to the Social Health Authority is the most consequential health reform in ageneration, promising predictable health financing, a functioning referral pathway and protectionfrom catastrophic expenditure. But its success will be decided not in Nairobi, but in the 47county health systems where citizens actually seek care.
The Social Health Authority operates within a comprehensive framework of health sectorreforms that include the Primary Health Care Act and the Facilities Improvement FinancingAct. These pieces of legislation are not stand-alone measures; rather, they form a coordinatedpackage designed to empower counties with both the mandate and the practical tools necessaryto deliver universal health coverage to every Kenyan. The Primary Health Care Actfocuses on strengthening community-level services, ensuring that preventive and basic curativecare reach even the most remote populations.
Meanwhile, the Facilities Improvement Financing Act provides counties with mechanisms tomobilise and utilise resources for upgrading health infrastructure, improving service quality andenhancing patient outcomes. Within this integrated system, SHA is expected to coordinateinsurance and payment mechanisms, regulate service delivery and ensure financial riskprotection for the population.
Success, therefore, hinges squarely on counties fulfilling theirresponsibilities. Any drift, neglect, or mismanagement at the county level will not merely impedeservice delivery but risk undermining the effectiveness of the entire reform agenda. Thestakes are high, and the performance of county governments is the decisive factor in turning thepromise of universal health coverage into a tangible reality for all Kenyans.
National reporting shows that while overall enrolment has grown, progress is uneven and somecounties lag significantly. Recent data revealed stark disparities. Garissa has registered only 2.3per cent of its population, Turkana just 3 per cent, Mandera 3.4 per cent, Wajir 4.1 per cent andWest Pokot 4.3 per cent. These figures are far counties below national standards, particularly inarid and semi-arid lands where service is most needed. By contrast, counties in central Kenyaand urban areas have recorded 18 to 20 per cent enrolment.
The Health Cabinet Secretary has acknowledged the registration gaps, citing poor connectivity,system glitches and weak infrastructure as barriers to uptake in remote areas. The Council ofGovernors has already signed an Intergovernmental Participatory Agreement with the Ministryof Health, providing the legal framework for counties to deliver SHA at the grassroots. Yet inmany areas this has not been translated into practice, and citizens continue to leave facilitiesunregistered.
Some counties are showing what is possible. Turkana launched a rapid results initiative thatregistered almost 100,000 residents in a week, offering temporary waivers on contributions andimproving its referral system. Uasin Gishu has also intensified outreach to expand coverage.
These examples prove that where there is political will and targeted mobilisation, registrationnumbers can rise quickly.
Every delay has consequences. A citizen turned away unregistered is not simply a numbermissing in the system. It is a patient denied treatment, a family pushed into debt, or a child goingwithout medicine. Beyond citizens, health workers are feeling the strain. Doctors, nurses andclinical officers report growing frustration at being unable to assist patients when services areinterrupted by registration failures or lack of cover. Staff are sometimes forced to improvise orturn people away, eroding trust, lowering morale and leading to overcrowding, burnout and adecline in service quality.
The Social Health Insurance Act requires universal registration, the Primary Health Care Actmakes community health promoters the entry point to the system, and the Facilities ImprovementFinancing Act allows facilities to retain revenue to stabilise basic services. Counties shouldalready be aligning their budgets and performance plans to these statutes. They should empowercommunity health promoters to register households at scale, ensure every facility is contractedand claims-ready, and use facility revenues to maintain operations.
The Intergovernmental Participatory Agreement signed by governors and the Ministry of Healthwas meant to codify how national and county actors share roles, data and accountability. Butsigning was only a first step. Implementation through joint work plans, measurable targets anddashboards is now required.
Counties must also address operational bottlenecks that citizens feel most sharply. They need toexpand household registration using mobile units, ward-level campaigns and market-day drives.
They must ensure facilities are able to submit clean claims promptly, with staff trained to use theSHA portal and equipped with proper ICT tools. Technical bottlenecks must be resolved quicklybecause a patient who queues all day only to be turned away may never return.
The Facilities Improvement Financing Act was created to keep facilities solvent for basics suchas utilities, repairs and buffer stocks. Counties should enact regulations where pending, enforcefinancial autonomy for facilities within the law and ensure revenues are spent on visible serviceimprovements. This will help keep clinics open and reliable even as reimbursements normalise.
Industrial action by doctors and clinical officers over the past two years has already disruptedservices and exposed gaps in human resource management. SHA cannot thrive if clinics areperiodically closed, if staff are casualised or if morale is brittle. Counties must resolveoutstanding labour issues, pay salaries on time and integrate SHA performance metrics such asclaims quality and service continuity into supervisory routines. The link between health workerconditions and patient experience is direct: when reimbursements are late, facilities rationservices and staff are stretched; when staffing is unstable, waiting times grow and referrals breakdown.
Citizens will judge reform not by legal frameworks or agreements but by what happens at thedispensary, the health centre and the county referral hospital. They will judge it by whetherregistration tables work, medicines are available, staff are present and claims are paid withoutdelay. National policy cannot rescue inertia at county level. Governors, county executives andchief officers must turn statutes and agreements into performance. They must enrol their people,contract their facilities, pay attention to data, protect their workforce and keep cash flowing tothe frontline.
If counties rise to this challenge, SHA will take root. If they do not, it will falter, and the mostvulnerable will pay the price.





Comments 0
Sign in to join the conversation
Sign In Create AccountNo comments yet. Be the first to share your thoughts!