
 The National Syndemic Diseases Control Council conducts free screening for non-communicable diseases like cancer on November 7, 2025. /NSDCC/X
The National Syndemic Diseases Control Council conducts free screening for non-communicable diseases like cancer on November 7, 2025. /NSDCC/X
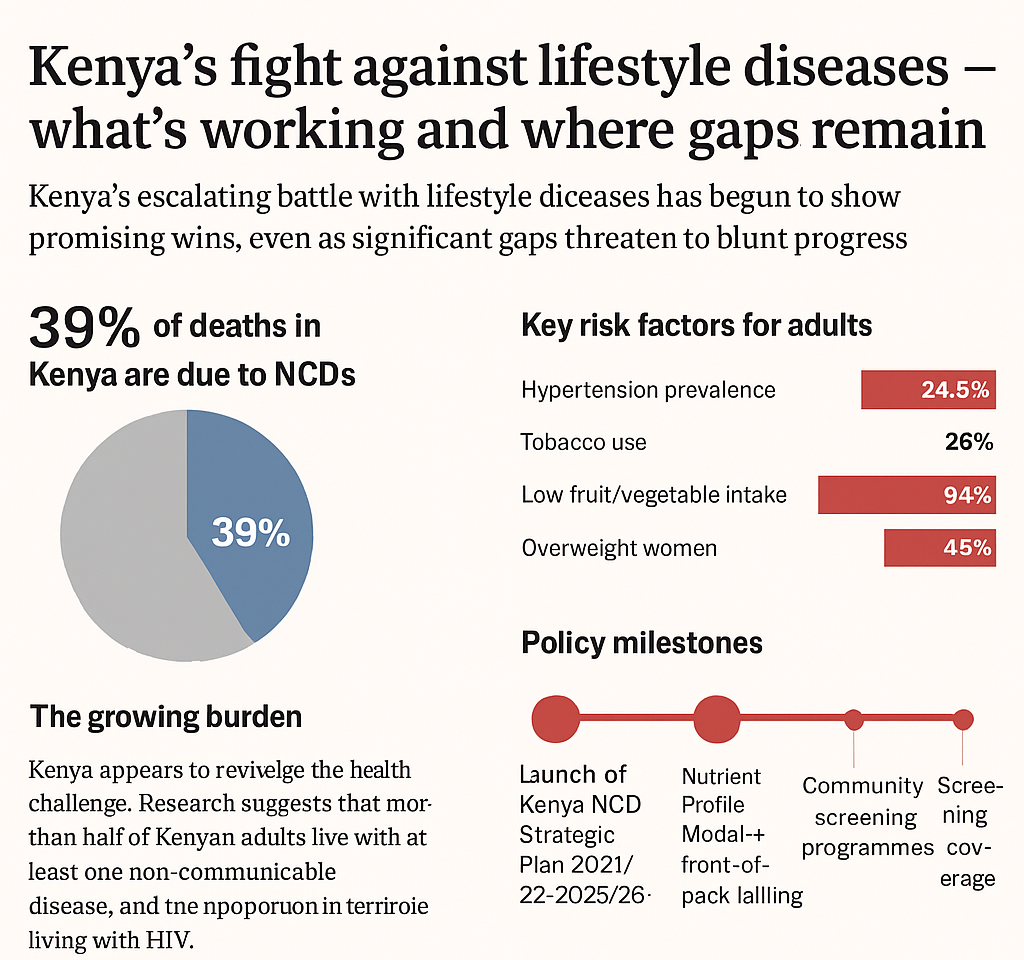
Kenya’s escalating battle with lifestyle diseases has begun to show promising wins, even as significant gaps threaten to blunt progress.
Non-communicable diseases (NCDs) now account for an estimated 39 per cent of all deaths in Kenya, reflecting a dramatic shift in the country’s health burden.
The major killers—heart disease, cancers, diabetes, and chronic respiratory conditions—are increasingly affecting younger, economically productive adults.
| Indicator | Value | Year/Source |
|---|---|---|
| Share of deaths in Kenya due to NCDs | 39% | Kenya National NCD Strategic Plan 2021/22–2025/26 |
| Prevalence of raised blood pressure (hypertension) in adults (18–69 years) | 24.5% | Kenya STEPS Survey 2015 |
| Among hypertensives: awareness | 29.4% | Kenya STEPS Survey 2015 |
| Children under five stunted | 18% | KDHS 2022 |
| Women aged 20–49 overweight | 45% | Ministry of Health Roundtable Aug 2025 |
| Tobacco use prevalence (overall) | 13.5% (males 19.9%, females 0.9%) | STEPS Survey 2015 |
| Adults whose fruit/veg intake <5 servings/day | 94% | STEPS Survey 2015 |
The growing burden
Kenya is confronting a rapidly evolving health challenge from non-communicable diseases.
Hypertension, which affects an estimated 20 per cent of adults, and high cholesterol are key drivers of the trend.
Research suggests that more than half of Kenyan adults live with at least one non-communicable disease, with the proportion even higher among persons living with HIV (62 per cent).
The 2025 Kenya Health Service Disruption Assessment Rapid Results Initiative Report by the National Syndemic Diseases Control Council (NSDCC) notes that cardiovascular diseases, diabetes, and chronic respiratory illnesses are the most prevalent NCDs among people living with HIV.
According to the report, diabetes coexists in approximately 10 – 15 per cent of tuberculosis (TB) cases, worsening treatment outcomes and increasing mortality risk.
Severe anaemia, malnutrition, and mental health disorders remain critical concerns, particularly among vulnerable groups such as adolescents and pregnant women.
“Cervical cancer, which is six times more common among HIV-positive women, remains the leading cause of cancer-related deaths in Kenya, with over 5,200 new cases and 3,800 deaths annually,” the report says.
At the same time, changes in diet, physical inactivity, and tobacco use are fuelling the epidemic. One study noted that NCDs accounted for about 35 per cent of all deaths, with nearly 22 per cent of those occurring before age 40.
The economic implications are stark. The 2021–26 national strategic plan warns that unless strong action is taken, the NCD burden will undermine Kenya’s universal health coverage aspirations and its economic growth.
What’s working
Kenya appears to be moving decisively on multiple fronts to tackle the NCD burden.
The government has outlined its commitment to ensuring health service equity, access, and sustainability through Universal Health Coverage.
The Digital Health Act, 2023, the Primary Health Care Act, 2023, and the Social Health Insurance Act, 2023 provide a robust platform for integrating and sustaining healthcare services.
The three Acts work together by establishing a framework for service delivery, an information system to connect services, and a financing mechanism to ensure access for all.
The Social Health Insurance Act, 2023 creates three distinct funds, including the Emergency, Chronic, and Critical Illness Fund, which serves as a safety net to cover costs associated with chronic and critical conditions such as cancer and MDR-TB after SHIF benefits are exhausted, preventing catastrophic out-of-pocket expenditures.
Further, the launch of the Kenya National NCD Strategic Plan 2021/22-2025/26 marked a key milestone.
The plan’s core focus is to achieve “a nation free from the preventable burden of NCDs.”
Its mission statement directs efforts to “halt and reverse the rising burden of NCDs through effective multisectoral collaboration and partnerships … ensuring Kenyans receive the highest attainable standard of NCD continuum of care that is accessible, affordable, quality, equitable, and sustainable, thus alleviating suffering, disease, and death for their well-being and socio-economic development.”
Among its specific targets are a one-third reduction in premature mortality from NCDs by 2025, a 30 per cent reduction in current tobacco use, a 15 per cent relative reduction in mean population salt/sodium intake, and screening coverage goals such as 20 per cent of women aged 40-75 years screened for breast cancer by 2025.
The government’s efforts are backed by tangible actions. In April 2023, the Ministry of Health, together with Development Gateway, launched a Tobacco Control Data Initiative dashboard giving policymakers real-time data on tobacco use.
Community- and primary-care-based approaches are also gaining traction. Interventions now emphasise early detection, screening, and integration of NCD services into the health system’s front line.
These moves signal a shift from disease treatment to prevention and systematic management.
Rural-urban and equity dynamics
While the national strategy highlights multisectoral action and equity, the lived reality shows stark differences between urban and rural Kenya.
Urban populations are more exposed to unhealthy diets, sedentary lifestyles, and processed foods—and risk factors such as overweight and obesity are higher in metropolitan settings.
Rural areas, meanwhile, often have lower access to screening and specialised care and may lag behind in awareness and treatment of NCDs. Such disparities matter.
If prevention, screening, and treatment remain concentrated in urban areas or among wealthier segments, the strategy’s promise of “equitable and sustainable” care may fall short.
The NCD burden is deeper within marginalised communities and at younger ages, undermining both health outcomes and socioeconomic potential.
Addressing rural access and urban risk issues side by side is thus critical for Kenya’s fight.
Gaps that still remain
Despite policy momentum, important gaps persist.
Financial constraints weigh heavily—treatment costs remain one of the greatest challenges for persons living with NCDs.
Workforce shortages, infrastructure deficits, and fragmented services in county systems continue to undermine access and continuity of care.
The donor-dependence trap
The recent shift in US foreign aid policy has had significant implications for Kenya, which depends heavily on donor funding for critical services such as TB treatment.
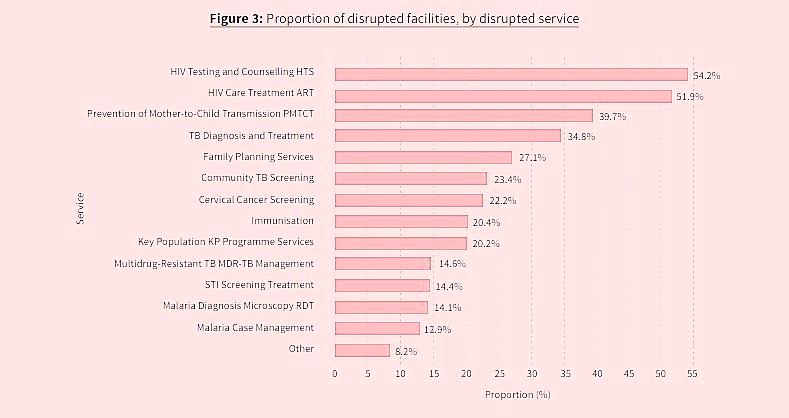
The Ministry of Health, through the NSDCC, undertook a Rapid Results Initiative (RRI) from April 1 to May 30, 2025, to evaluate the impact of service disruptions caused by the withdrawal of US government support.
The census-based survey conducted across all 47 counties created Kenya’s most complete portrait of health system fragility.
It showed that the withdrawal of US funding triggered widespread service disruptions across Kenya’s health system, with 40.6 per cent of facilities (2,127 out of 5,245) reporting significant interruptions in care delivery.
Rural facilities bore the brunt, with 1,875 (51.1 per cent) affected.
“TB diagnosis and treatment were disrupted in 34.8 per cent of facilities, with Turkana and Marsabit counties experiencing near-total system failure in TB care,” the RRI report showed.
The funding withdrawal also triggered a healthcare workforce crisis.
Some 39.5 per cent of disrupted facilities (841 sites) reported critical staff withdrawals, primarily affecting nurses and clinical officers, who constituted 68 per cent of departed staff.
The RRI report indicated that nurse-to-patient ratios worsened catastrophically from 1:50 to 1:120 in high-burden counties like Kakamega.
“In facilities retaining staff, 44.4 per cent (944 sites) documented dangerous workload surges, forcing consultations to be truncated to under five minutes per patient—a 67 per cent reduction from pre-withdrawal standards.”
The RRI also found that the withdrawal of US aid triggered medicine and commodity stockouts in affected facilities, with the stockout rate of TB preventive therapy hitting 13.7 per cent.
Turkana and Marsabit counties were most affected, leading to increased paediatric TB cases.
At least 38 counties (80.9 per cent) depended on donor funding for more than half of their HIV, TB, and malaria programme budgets.
“This heavy reliance created severe vulnerability, with 74.5 per cent of counties forced to deprioritise HIV/TB programmes when reallocating scarce domestic funds.”
In response to the crisis, the RRI showed that 14 counties (29.8 per cent) introduced user fees for services that were previously free, placing additional burdens on patients amid SHIF systemic instability.
Low data to guide interventions
Surveillance and up-to-date data also pose a problem: many risk-factor surveys date back to 2015, limiting the ability to monitor progress accurately.
Coverage of screening and treatment remains sub-optimal. For example, hypertension control is still far below the target set in the strategic plan.
The food environment presents another barrier—ultra-processed foods, rising sugar intake, and weak regulation continue to drive diet-related risk.
The 2015 Kenya Stepwise Survey found that only five per cent of adults consume the WHO-recommended five servings of fruits and vegetables per day.
The average intake is just two servings, while 19 per cent of adults consume none at all.
Further, the 2022 Kenya Demographic Health Survey (KDHS) indicated that only 49 per cent of women meet minimum dietary diversity. Seventy per cent regularly consume sweetened beverages and 35 per cent eat unhealthy foods.
"Diets are still cereal-heavy, while myths, misinformation and unchecked marketing of unhealthy foods worsen the situation,” Veronica Kirogo, Head of the Division of Nutrition and Dietetics at the Ministry of Health said in a story carried by the Star in September.
Rirogo said despite significant progress in improving nutrition over the past two decades, Kenya continues to face a triple burden of malnutrition with anaemia at 41.6 per cent among pregnant women and 26.3 per cent among preschool children.
Country director of the Global Alliance for Improved Nutrition, Ruth Okowa, warned that alongside undernutrition, overweight and obesity are rising rapidly.
“More Kenyans, both young and old, are now at risk of diet-related non-communicable diseases such as cancer, diabetes, hypertension and cardiovascular diseases,” she said.
The way forward
Speaking during the launch of the Kenya National NCD Strategic Plan (NSP) 2021/22-2025/26 in July 2021, Dr Mercy Mwangangi, currently CEO of the Social Health Authority (SHA), noted that Kenya stood at a pivotal point in its health journey.
She said to turn the strategy’s goals into outcomes, the planned multisectoral, population-wide interventions must be fully implemented and scaled.
“The development of the Kenya National NCD Strategic Plan (NSP) 2021/22-2025/26 is informed by the need to strengthen a comprehensive multisectoral response to the increasing NCD burden,” she said.
The strategic plan provides a sound roadmap, and pockets of implementation are showing promise.
However, the ambitious targets will only be met if the gaps highlighted earlier on are addressed.
Success would mean fewer premature deaths from NCDs, equal access to screening and care for all Kenyans, and healthier communities with reduced costs for both individuals and the economy.
According to the 2014 KDHS, Kenya loses an estimated Sh373.9 billion annually, which is 6.9 per cent of GDP, due to malnutrition-related health, education and productivity losses.
What lies ahead is a test of execution, equity and system-wide alignment—a fight Kenya can win if it keeps the momentum.







Comments 0
Sign in to join the conversation
Sign In Create AccountNo comments yet. Be the first to share your thoughts!