
Kenya’s health sector is entering a year of change, driven by new funding arrangements, ongoing reforms to national health insurance, labour unrest among health workers and rapid adoption of digital technologies.
Many of the shifts taking shape now will directly affect how Kenyans access care, how services are funded and who delivers them.
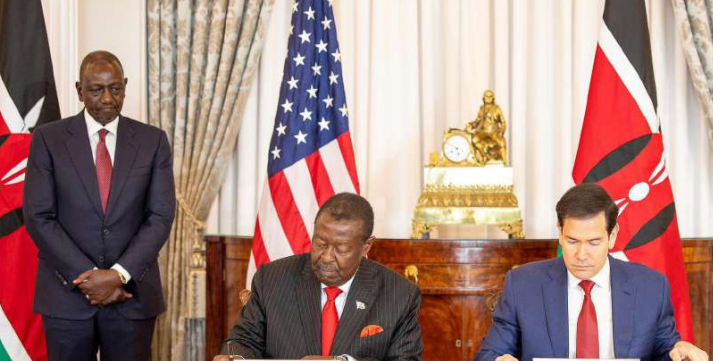
One of the biggest developments is the Kenya–United States Health Cooperation Framework, signed in Washington on December 4, 2025.
The five-year agreement is expected to channel $1.6 billion (Sh208 billion) into Kenya’s health system over five years, beginning April this year.
The country is currently in a transition, which ends March 31 this year, marking a complete departure from how American health funding has historically been delivered.
The framework says “the United States will invest directly in government health institutions and not NGOs”. This represents a clear shift away from the long-standing model under which programmes such as the US President's Emergency Plan for Aids Relief (Pepfar) and Usaid operated largely through international and local non-governmental organisations.
President William Ruto said the agreement supports the Kenya Kwanza health agenda.
“The framework we sign today adds momentum to my administration’s universal health coverage that is focused on supply of modern equipment to our hospitals, efficient and timely delivery of health commodities to our facilities, enhancement of our health workforce, and health insurance for all, and leaving no Kenyan behind,” he said.
Other Kenyan officials have described it as a major policy shift. Medical Services PS Ouma Oluga said, “This framework represents a departure from previous approaches and is expected to have a lasting impact on health for all.”
Since 2003, Pepfar has been central to Kenya’s HIV response, supporting treatment programmes, laboratories, health workers and community outreach.
Under the new arrangement, funds will flow directly to Kenyan government systems, placing more responsibility on national and county institutions to plan, manage and account for spending. It also means many NGOs that have worked in the health sector for decades are likely to see their roles reduced or redefined.
However, the agreement has not moved forward smoothly.
Last month, the High Court issued a conservatory order suspending parts of the framework following a petition that raised concerns about data protection and public participation.
The court ordered that “the respondents are restrained from implementing or giving effect to the Health Cooperation Framework executed between the Government of Kenya and the Government of the United States of America.”
The case has focused on whether the agreement allows sharing of sensitive health data without adequate safeguards.
Health CS Aden Duale has defended the framework, saying it does not permit the transfer of personally identifiable data and arguing that Kenya retains control over its health systems.
On the other hand, 2026 is the second year of the Social Health Authority (SHA), which replaced NHIF as the main vehicle for delivering universal health coverage in Kenya.
By mid-2025, more than 24 million Kenyans had been registered under Taifa Care. CS Duale said the programme is designed to reduce out-of-pocket spending for patients.
“This fund is budgeted, appropriated by Parliament, and paid to the Ministry of Health to ensure ordinary Kenyans receive the healthcare they need without paying from their pockets,” he said.
Primary healthcare has been a key focus of the new system.
In 2025, the government announced that services at public primary care facilities would be provided free of charge, with the aim of easing pressure on households and reducing delays in seeking treatment.
But the rollout of SHA has also exposed weaknesses.
Fraud and abuse of the system have been flagged, particularly through digital claims processing. In December 2025, dozens of facilities were suspended over fraudulent claims.
“These activities undermine public trust in our health system and threaten the feasibility and sustainability of the Social Health Authority,” Duale said.
At the same time, Kenya is expanding its digital health infrastructure. In August 2025, the Ministry of Health launched the Digital Health Agency’s strategic plan.
Duale said the government was rolling out the “Taifa Care Digital Platform – integrating electronic health records, telemedicine, insurance management, and facility data to ensure continuity of care, prevent fraud and improve patient experience”.
Digital tools are also being paired with new technologies, including artificial intelligence. In 2025, the ministry supported the introduction of AI-powered diagnostic equipment, including a 256-slice CT scanner.
“As we embrace AI and advanced diagnostics, we must not lose sight of our responsibility to ethical practice, sustainability, and equitable access to care,” Dr Tom Menge, director of Health Products and Technologies, said at the launch.
The government’s National AI Strategy 2025–30 places health among the key sectors expected to benefit from data-driven systems, predictive analytics and automated processes.
These tools are likely to be used more widely for diagnostics, disease surveillance and claims verification in 2026, even as concerns about data protection and access remain.
While policy reforms and technology are advancing, labour relations continue to pose a challenge. Strikes by clinical officers, nurses and doctors disrupted services in several counties in 2025, with disputes centred on pay, career progression, working conditions and delayed payments under the new insurance system.
The Kenya Union of Clinical Officers (Kuco) members are currently on strike.
Kuco general secretary and CEO George Gibore said the government had failed to honour a return-to-work agreement signed on July 8, 2025, as well as another pact concluded with the Ministry of Health on July 27, 2024.
Both agreements, he said, were meant to clear the way for signing, registering and implementing the CBA.
“It is most unfortunate and concerning that despite parties having concluded the negotiations, the Ministry of Health is reluctant to sign the same so as to pave way for court registration and implementation,” he said.
CS Duale has criticised the industrial actions by medics. In one statement, he said, “Union leaders are turning a very noble healthcare workforce… into a tool for their own games.”
Looking back, 2025 also recorded some gains.
Aden Duale was reassigned from the Ministry of Environment to the Ministry of Health on March 26, 2025.
Former Health CS Deborah Barasa was moved to the Ministry of Environment.
Under Duale, the Ministry of Health expanded enrolment under Taifa Care, increased funding for primary health services and took steps to address fraud and inefficiencies.
The CS said the government had allocated Sh13 billion for primary healthcare and Sh6.2 billion for UHC contract health workers, signalling continued investment in frontline services.
Other health pressures are expected to persist into 2026. Mental health needs continue to rise, while non-communicable diseases such as diabetes and hypertension account for a growing share of clinic visits, according to the Ministry of Health. Counties also face ongoing challenges in financing health services amid competing budget demands.
For patients, the year ahead will likely bring a mix of improvements and uncertainty. Expanded insurance coverage and free primary care could reduce financial barriers, while new technologies may improve diagnosis and efficiency. At the same time, strikes, court battles and system weaknesses could disrupt services.







Comments 0
Sign in to join the conversation
Sign In Create AccountNo comments yet. Be the first to share your thoughts!